Acute Cholecystitis: Early Signs, Symptoms, and Modern Diagnostic Approaches
By Dr. Ahmad Elwahidi, Consultant General Surgery
Acute cholecystitis, an inflammation of the gallbladder, is a common and potentially serious condition that requires timely diagnosis and intervention. As a consultant in general surgery, I often encounter patients with this condition, and in this blog, I will outline its early signs, symptoms, and the evolving approaches to its diagnosis.
What is Acute Cholecystitis?
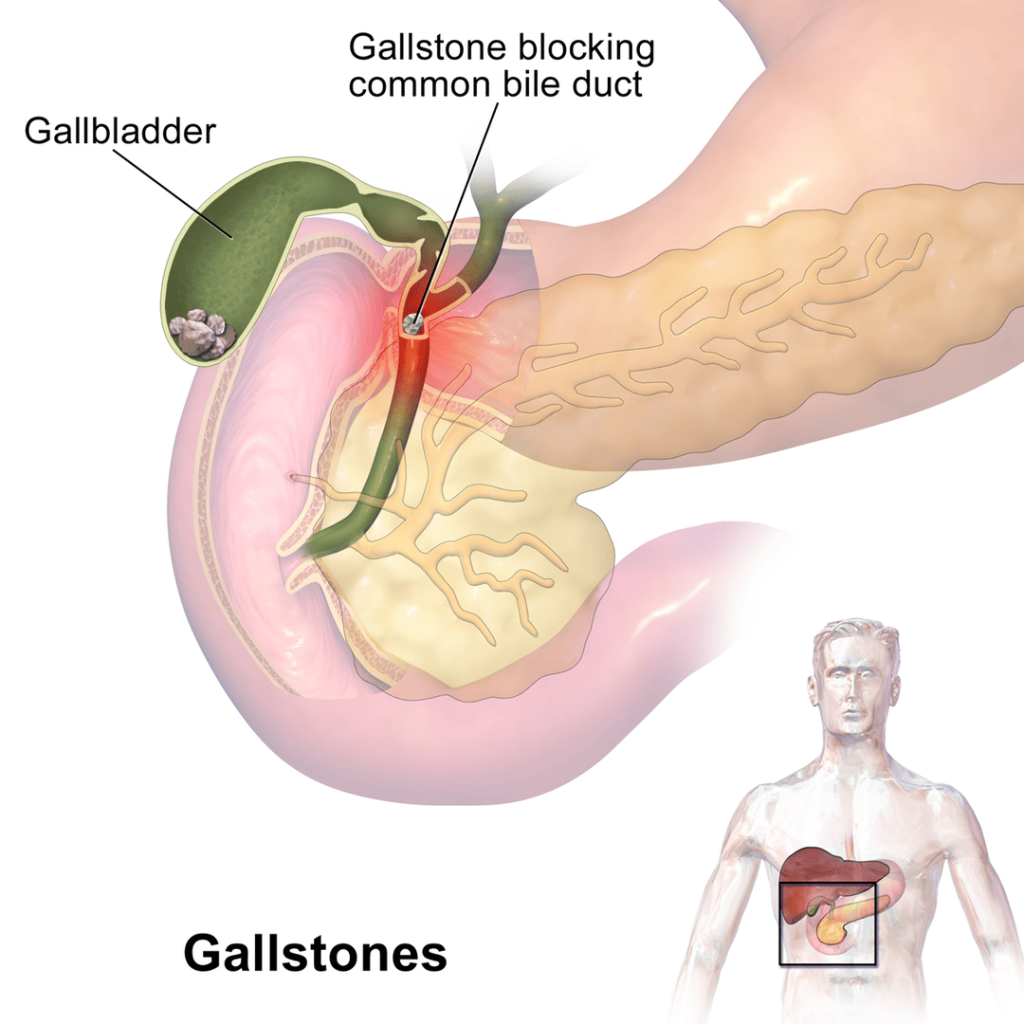
The gallbladder, a small organ beneath the liver, stores bile produced by the liver to aid in digestion. Acute cholecystitis usually arises when gallstones block the cystic duct, resulting in inflammation. In some cases, the inflammation can occur without gallstones (acalculous cholecystitis), which is more common in critically ill patients.
If left untreated, acute cholecystitis can lead to complications such as gangrene, gallbladder perforation, and peritonitis, necessitating immediate medical attention.
Early Signs and Symptoms
Recognizing the early signs of acute cholecystitis is critical for timely diagnosis and treatment. Patients typically present with:
- Right Upper Quadrant Pain: The most common symptom is a sudden and intense pain in the upper right side of the abdomen. The pain may radiate to the right shoulder or back.
- Tenderness and Guarding: Upon physical examination, tenderness in the right upper quadrant is common. Murphy’s sign—a sudden stop in inspiration upon palpation of the gallbladder—is a classical clinical finding.
- Fever and Chills: Inflammation of the gallbladder often triggers fever, a sign of infection.
- Nausea and Vomiting: Many patients experience digestive symptoms like nausea and vomiting, especially after consuming fatty foods.
- Jaundice: In some cases, when the bile duct is obstructed, jaundice (yellowing of the skin and eyes) may develop, although this is more common in choledocholithiasis.
New Approaches to Diagnosis
Traditionally, diagnosing acute cholecystitis relied heavily on clinical examination and basic imaging techniques such as ultrasound. While these remain invaluable tools, advancements in diagnostic modalities have enhanced the accuracy and speed of diagnosis. Here’s a look at modern approaches:
- Enhanced Ultrasonography: Ultrasound remains the first-line imaging technique, offering a quick and non-invasive method to detect gallstones and assess gallbladder wall thickening, pericholecystic fluid, and sonographic Murphy’s sign. Doppler ultrasonography can also assess gallbladder blood flow, providing critical information in severe cases.
- Hepatobiliary Iminodiacetic Acid (HIDA) Scan: When ultrasound results are inconclusive, a HIDA scan can confirm acute cholecystitis. This nuclear medicine test evaluates the functionality of the gallbladder and can identify cystic duct obstruction, which is a hallmark of the disease.
- Magnetic Resonance Cholangiopancreatography (MRCP): MRCP offers a non-invasive, highly detailed visualization of the biliary and pancreatic ducts. It is particularly useful in diagnosing acute cholecystitis when there is suspicion of concurrent common bile duct stones.
- CT Scan: While not routinely used as the first imaging option, a CT scan can reveal complications such as gangrene, perforation, or emphysematous cholecystitis. In some centers, CT is increasingly used in critically ill patients.
- Point-of-Care Ultrasonography (POCUS): In emergency settings, POCUS is gaining popularity as a bedside tool that allows quick identification of gallbladder issues, helping clinicians make faster decisions in acute cases.
- Biomarkers and Lab Tests: Inflammatory markers such as white blood cell count (WBC), C-reactive protein (CRP), and liver function tests (LFTs) support the diagnosis, especially when used alongside imaging.
A Modern Approach to treatment
The diagnosis of acute cholecystitis has evolved with advancements in technology, allowing for quicker and more accurate detection. Once diagnosed, the treatment typically involves intravenous antibiotics to treat infection and fluid resuscitation. Surgery, usually a laparoscopic cholecystectomy, is the definitive treatment for most cases. Advances in minimally invasive surgery have significantly reduced recovery times and complications.
In select cases of acalculous or complicated cholecystitis, percutaneous cholecystostomy (inserting a tube to drain the gallbladder) can be performed as a temporizing measure in critically ill patients who are not fit for surgery.
Acute cholecystitis is a potentially life-threatening condition that demands prompt attention. The combination of early recognition of symptoms and the application of modern diagnostic tools allows for better patient outcomes. As imaging techniques and diagnostic modalities continue to evolve, we are better equipped to treat this condition efficiently.
If you or someone you know experiences symptoms that could indicate acute cholecystitis, seeking medical advice early is critical. As a consultant general surgeon, I can emphasize that early intervention not only alleviates pain but also prevents serious complications.